
Conductive hearing loss is hearing loss caused by a physical blockage or damage in the outer ear, ear canal, eardrum, or the small bones of the middle ear.
Sound cannot travel efficiently to the inner ear, so voices and everyday sounds feel muffled, distant, or quieter than usual.
Most cases are treatable, and many resolve completely once the underlying cause is addressed (wax, infection, fluid, or a structural problem).
In Australia, conductive hearing loss is the most common type of hearing loss in children, largely because of middle ear infections and glue ear (AIHW, 2024).
In adults, it is the type most often behind a sudden or temporary hearing change after a cold, a flight, or wax build-up. The good news: it is also the type most likely to be reversed with the right hearing loss treatment.
What Is Conductive Hearing Loss?
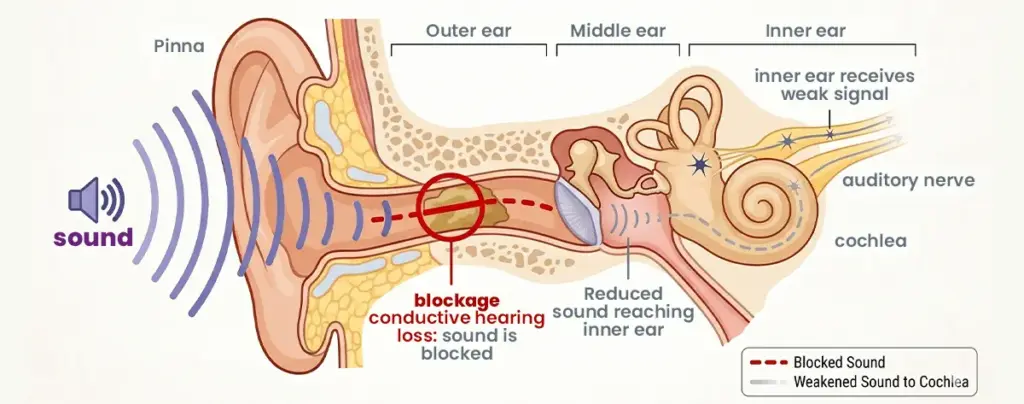
Conductive hearing loss (CHL) is a mechanical hearing problem. Sound waves cannot move efficiently through the outer or middle ear into the inner ear, leading to conductive hearing loss.
The inner ear and auditory nerve are working normally. The problem sits in the conduction pathway that delivers sound to them.
This is the key distinction from sensorineural loss, where the cochlear hair cells or auditory nerve itself are damaged.
Conductive losses are usually partial and very often reversible. People can still hear, just less well.
Three structures can be affected:
- The outer ear: pinna and ear canal
- The eardrum (tympanic membrane): the thin membrane that vibrates with sound
- The middle ear: the air-filled space containing the malleus, incus, and stapes (the ossicles), plus the Eustachian tube that drains it
The 6 Main Causes of Conductive Hearing Loss
Most cases fall into one of six categories. The causes of hearing loss determines the treatment, so identifying it accurately matters.
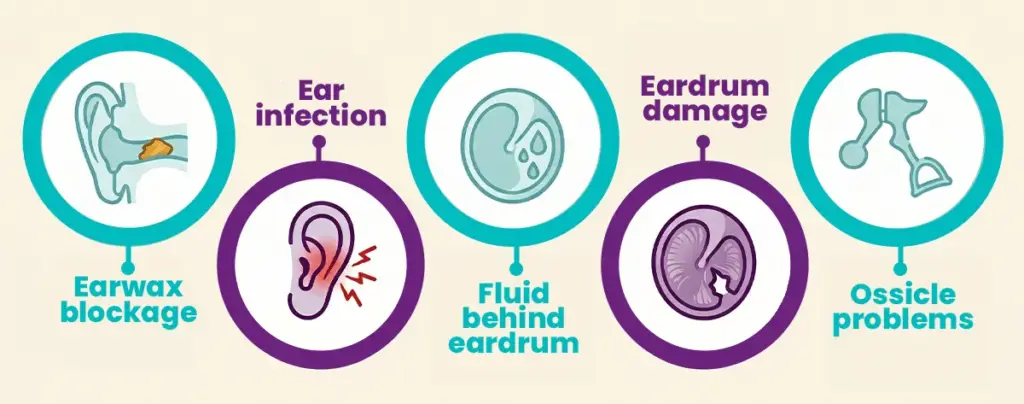
1. Earwax (cerumen) impaction. A blocked ear canal is a leading cause of conductive hearing loss in adults and is fully reversible with professional cleaning.
2. Middle ear infection (otitis media). Bacterial or viral infection causes fluid and pressure to build up behind the eardrum. Very common in children under five.
3. Glue ear (otitis media with effusion). Sticky fluid stays trapped in the middle ear long after an infection has cleared. Often follows a cold or allergy flare-up.
4. Perforated eardrum. A hole in the tympanic membrane caused by infection, sudden pressure change (a slap, an explosion, deep diving), or a cotton bud injury.
5. Otosclerosis. Abnormal bone growth around the stapes prevents it from vibrating freely. Often hereditary and typically presents between 20 and 40 years of age.
6. Structural or congenital issues. A narrowed or absent ear canal (aural atresia), benign growths such as cholesteatoma, or damage to the ossicles from trauma.
Less common causes include foreign objects in the ear canal (especially in children), swimmer’s ear (otitis externa), and tumours of the middle ear.
Symptoms: What Conductive Hearing Loss Feels Like
The hearing change is the obvious symptom of hearing loss, but the texture of it is distinctive. Typical symptoms include:
- Muffled sounds, as if the ear is plugged or under water
- A persistent feeling of fullness or pressure in one or both ears
- Difficulty hearing soft voices, while loud sounds remain tolerable (often surprisingly clear)
- Your own voice sounding louder or hollow inside your head, a phenomenon called autophony
- Ear pain, drainage, or tenderness when an infection is the cause
This is the opposite of sensorineural hearing loss, where noise makes things worse.
Conductive vs Sensorineural Hearing Loss
The treatment paths diverge sharply, so the distinction matters. Conductive loss is mechanical and often reversible. Sensorineural loss is nerve-related and usually permanent.
| Feature | Conductive | Sensorineural |
| Where the damage is | Outer or middle ear | Inner ear (cochlea) or auditory nerve |
| Reversibility | Often reversible | Usually permanent |
| First-line treatment | Medical or surgical | Hearing aids |
| Audiogram pattern | Air-bone gap of 15 dB or more | Air and bone thresholds roughly equal |
| Speech clarity | Usually preserved (quieter, not garbled) | Often distorted, especially in noise |
| Most common in | Children with ear infections, adults with wax | Adults over 60, noise-exposed workers |
Mixed hearing loss exists too: a conductive component (such as glue ear) layered over an underlying sensorineural hearing loss. The treatment plan addresses each layer separately.
How an Audiogram Shows Conductive Hearing Loss
An audiogram plots the quietest sounds you can hear (in decibels) across a range of frequencies (in hertz). For conductive hearing loss, the diagnostic signature is the air-bone gap.
Two thresholds are measured:
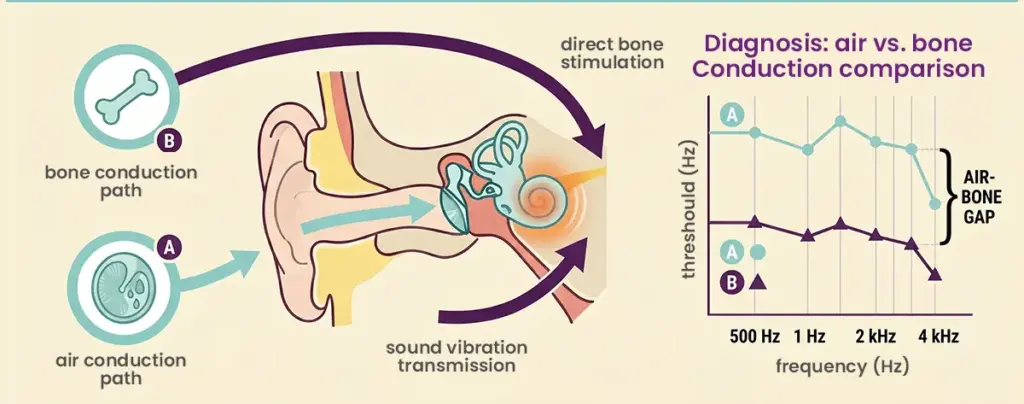
- Air conduction: uses headphones or insert earphones. Tests the full pathway (canal, eardrum, middle ear, inner ear, nerve).
- Bone conduction: uses a small vibrator placed on the mastoid bone behind the ear. Bypasses the outer and middle ear and tests the inner ear and nerve directly.
When bone conduction is normal but air conduction is worse, the gap between the two lines is the air-bone gap.
A gap of 15 dB or more across two or more frequencies is the clinical definition of a conductive component.
On the chart, this appears as a clear vertical separation between the air conduction line (poorer thresholds) and the bone conduction line (normal or near-normal), on the side of the affected ear.
The bigger the gap, the more conductive the loss.
How Conductive Hearing Loss Is Diagnosed in Australia
Diagnosis follows a standard pathway. Most cases can be resolved without ever needing a hospital referral.
Step 1: Otoscopic examination. A clinician looks inside the ear canal and at the eardrum using an otoscope. Wax, fluid, perforations, or infection are identified visually.
Step 2: Tympanometry. A small probe measures eardrum movement and middle ear pressure. It is the fastest way to detect fluid behind the eardrum and a stiff or perforated drum.
Step 3: Pure-tone audiometry. The formal hearing test that produces the audiogram. Identifies both the degree and the type of hearing loss.
Step 4: Tuning fork tests (Weber and Rinne). A quick clinical check that confirms whether the loss is conductive or sensorineural. Often done by GPs before a referral.
Step 5: ENT referral when needed. Persistent fluid, recurrent infections, suspected otosclerosis, or any structural concern is referred to an ear, nose and throat (ENT) specialist for imaging or surgical assessment.
In Australia, adults can usually access an audiologist directly without a GP referral. Eligible adults can also access subsidised assessment through the Hearing Services Program.
A free hearing check is the easiest way to start.
Treatment Options for Conductive Hearing Loss
Treatment depends entirely on the cause. The general principle: fix the underlying problem first, and only consider hearing devices when the cause is permanent or cannot be safely treated.
- Earwax removal. Microsuction or curette removal by a qualified clinician. Do not use cotton buds at home, which usually push wax further in.
- Antibiotics or antifungal drops. For active middle ear or ear canal infections.
- Watchful waiting. For mild glue ear in children, fluid often clears within three months without intervention, in line with international clinical guidelines.
- Grommets (ventilation tubes). Small tubes inserted through the eardrum to drain persistent fluid. Routine day surgery in Australia.
- Tympanoplasty. Surgical repair of a perforated eardrum. Usually performed when the perforation has not healed within a few months.
- Stapedotomy or stapedectomy. Microsurgery that frees the fixed stapes bone in otosclerosis by replacing it with a small prosthesis. Performed by an ENT surgeon under general anaesthetic.
- Hearing aids. Used when the conductive loss is permanent (untreatable otosclerosis, chronic middle ear disease).
- Bone-anchored hearing systems (BAHA). A device that transmits sound through the skull bone directly to the inner ear. Particularly useful for single-sided hearing loss, chronic ear infections, and aural atresia.
Are Hearing Aids Used for Conductive or Sensorineural Hearing Loss?
Hearing aids are designed primarily for sensorineural hearing loss, which is permanent and far more common. They are, however, also a valid treatment for conductive hearing loss when surgery is not an option or not preferred.
A conventional hearing aid works by amplifying sound. This compensates for the reduced volume reaching the inner ear.
Conductive losses leave speech clarity largely intact, which generally makes amplification straightforward to adapt to for those who choose hearing aids over surgery.
When a conventional aid is unsuitable (a chronically draining ear, a closed-off canal, or a single-sided conductive loss), bone-anchored systems are the preferred option. They bypass the outer and middle ear entirely and deliver sound through bone vibration directly to the cochlea.
If you are not sure which approach suits your case, browse the types of hearing aids or book a free hearing aid trial.
When to See a Hearing Specialist
Book a hearing assessment if any of the following applies:
- Hearing has changed and not returned to normal within two weeks.
- There is ongoing pain, drainage, or pressure in the ear.
- Hearing dropped suddenly within the past 72 hours. This is a medical emergency: see your GP or attend an emergency department.
- A child is not responding to sound as expected, has frequent ear infections, or has unclear speech for their age.
- You have persistent dizziness or tinnitus alongside the hearing change. See our guide on ringing ears and tinnitus for more.
Most conductive hearing losses are simple to identify and very treatable when caught early.

